From Panel to Protocol
Eight compounds. Six months. Twenty-one weekly injections distributed across six active days. The locked-in elite biohacker protocol — fully instrumented, fully reversible, fully documented.
Eight compounds. Six months. Twenty-six million pesos. A locked-in elite biohacker protocol assembled with a Bogotá endocrinologist via TRT Colombia, fully instrumented for measurement, fully reversible, fully documented.
This is the final state of the biohacker stack assembled with TRT Colombia under Dr. José Luis Barrera Orozco — endocrinologist, prescription dated April 27, 2026. The full picture: hormonal optimization, metabolic reset, growth-hormone stimulation, tissue repair, cellular energy, anti-aging.
This is the operating reference for the protocol — what is in it, what each compound does, what it costs, how it gets stored, how it gets monitored, where it sits on the spectrum of compound-based optimization.
The stack
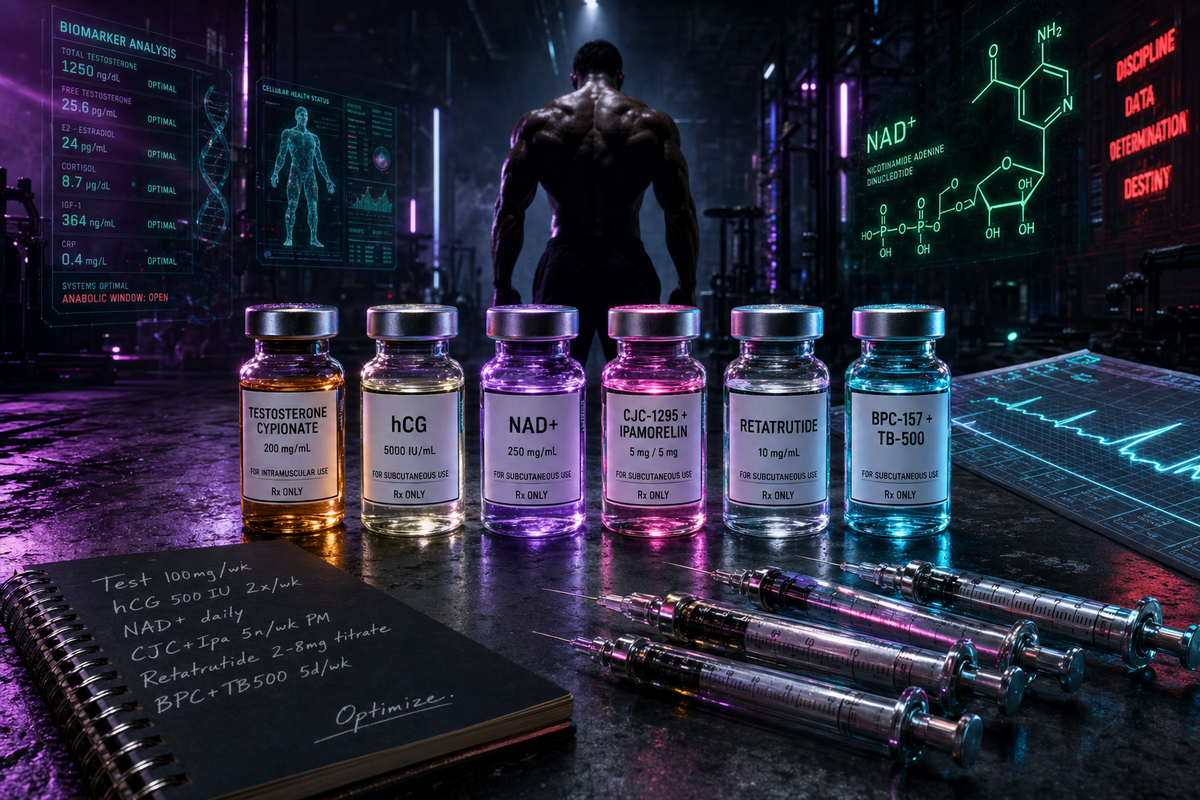
Eight compounds organized across five layers — hormonal foundation, growth hormone axis, fat loss and metabolic, tissue repair, cellular energy and longevity. Hormones run six months. Peptides cycle for three, with re-order option after the 12-week bloodwork checkpoint.
All compounds delivered with bacteriostatic water plus ten syringe kits per vial. Testosterone ships with syringes only — no reconstitution needed for an oil-based intramuscular preparation.
The cost
Full transparency on the locked-in protocol pricing in Colombian pesos and US dollar equivalent at 4,000 COP per dollar. Every compound includes its consumables. Optional medicine case and nurse training added separately.
Compound stack: 26,520,000 COP. Add 4 nurse visits across Day Zero week (800,000 COP), one medicine case with cold ice gel for travel (95,000 COP — second case included free), and a 5% bulk-order discount on the consolidated transfer (−1,370,750 COP). The TRT storage vial container is also included free.
Final transfer to TRT Colombia: 26,044,250 COP / ~$6,511 USD.
Plus already paid: $555.59 USD in Amazon-sourced Day Zero infrastructure (Pelican case, AstroAI mini fridge, sharps containers, sterile vials, vial spikes, OMRON BP+EKG, travel case).
Day Zero ALL-IN: ~$7,067 USD for six months of fully-instrumented compound-driven optimization with home nurse training, cold-chain delivery, and complete Day Zero infrastructure.
What seven thousand dollars actually unboxes — the full eight-compound stack delivered, organized, and ready for Day Zero:
The schedule
The protocol opens with a four-visit nurse training week at the home, locked into the order at 200,000 COP per visit. Compounds arrive separately via clinic delivery driver with cold-chain handling — ice gel packs in transit — guaranteed before the nurse arrives. First visit walks through every injection type hands-on (testosterone IM, peptides subQ, NAD+ subQ, HCG subQ), prepares and mixes the medications, administers the first dose. The clinic provides step-by-step manuals plus video instructions for ongoing reconstitution. Across the rest of the training week technique gets dialed in across each compound. Solo execution from there with a WhatsApp clinic backstop.
Re-evaluation gate: 8-12 week bloodwork retest — same lab, same prep, same tubes. Full panel: glucose (fasting and post-load), insulin (fasting and post-load), HbA1c, ALT, AST, lipid panel, TSH, Free T4, CBC, estradiol, PSA, vitamin D 25-OH, total and free testosterone, creatinine, ferritin, serum iron, SHBG, IGF-1.
Re-order decision happens at the 12-week mark based on what those numbers say. Hormones already locked for six months; peptides re-order optional based on results.
Storage
Two buckets and the warm-climate rule from TRT Colombia.
Room temperature (Pelican 1200, dark closet, 15-25°C): Testosterone Cypionate — never refrigerate, oil thickens. Sealed bacteriostatic water. Syringes, alcohol pads, supplies.
Refrigerator (AstroAI 6L dedicated, 2-8°C): all peptides regardless of state. Sealed dry powder vials of HCG, NAD+, Retatrutide, CJC-1295, Ipamorelin, BPC-157, TB-500 go in cold storage on arrival under the warm-climate rule. Once reconstituted, they stay in the fridge — HCG, Retatrutide, NAD+ keep about 30 days; CJC-1295, Ipamorelin, BPC-157, TB-500 keep 14-30 days depending on the molecule. Opened bacteriostatic water also moves to the fridge.
The Medellín climate rule (TRT Colombia guidance for warm climates 22-28°C): Testosterone = Pelican room temp always. ALL peptides = AstroAI fridge whether sealed or reconstituted. Never pre-mix the whole stack — degrades faster than it can be used. Reconstitute one vial at a time.
The setup
$560 USD all-in for Day Zero infrastructure across seven Amazon items plus local Rappi sourcing of alcohol prep pads.
The clinic provides the consumables side: bacteriostatic water and ten syringe kits per compound order, plus the medicine case with cold ice gel for travel. Everything else is the operator's responsibility — and now sourced.
Monitoring
Three signal layers running in parallel: continuous Oura Ring telemetry (HRV, resting HR, sleep stages, body temperature, stress score), daily AM blood pressure and single-lead EKG via OMRON Complete, and quarterly DEXA body composition scans in Medellín.
Tag taxonomy in Oura: every injection logged with compound name, time, body site, and any acute side-effect signal. The pattern recognition layer catches anomalies — sleep regression after a specific peptide, HRV drop after a CJC night, BP creep over weeks of testosterone.
Bloodwork checkpoint: week 12 of the protocol. Same lab as the panel baseline. Side-by-side delta on every marker. That's the gate where doses adjust, peptides re-order or rotate, and the second half of the year locks in.
Where this sits
There is a rough hierarchy in compound-based optimization. Useful to know where this stack lands.
This stack lands in upper Tier 3, edging into Tier 4 with NAD+ and Retatrutide added. Above 95% of TRT clinics' standard prescriptions. Below the AAS-stacking territory of competitive bodybuilders. Quantified, monitored, doctor-supervised, fully reversible.
What this stack deliberately is not: Tier 5 territory. No trenbolone, no deca, no anadrol, no polypharmacy escalation. Every compound has a clinical rationale, a measured endpoint, and a 12-week off-ramp built in.
The execution
The framework is set. The compounds are in. The nurse training is scheduled. The supplies are sourced. The instrumentation is calibrated. The retest is on the calendar.
Six months of structured optimization with a 12-week bloodwork checkpoint. Documented end to end. Public log running.
From panel to protocol. Locked in.
Related Reading
- Recalibration Day
- From Protocol to Practice
- Panel Says Go. Time to Push.
- Baseline Drawn: One Clean Night, Blood on the Table
- Choosing a Biohacking Clinic in Medellín
- Final NAD+ Adjustment
- The Wolverine Stack — the BPC-157 + TB-500 repair stack — how it heals, the availability-over-mass reframe for lifters, and the honest evidence + legal reality.
- Blast & Cruise — the testosterone strategy — TRT vs blast ranges, timing, the ancillary stack, and a 250mg blast from a 100mg base.
- The Dashboard on Your Forehead
- Split the Shot
- Three Days of Nothing



